Masquelet Technique
The Masquelet technique is a technique used by Mr SInha and Mr Daurka for the treatment of large bone defects.
The technique involves the insertion of an antibiotic loaded polymethylmethacrylate (PMMA) bone cement spacer into the area of bone loss. The bone is stabilised by internal fixation with plate and screws, an intramedullary rod or external fixation.
The cement spacer stimulates a biological membrane to form around it. This membrane has been shown to contain bone morphogenic proteins (BMPs) and growth factors (GFs) which are important in bone hearing.
Between 6 and 10 weeks after implantation of the cement spacer the biological membrane has peak concentrations of the BMPs and GFs.
This is the optimum time to perform the second stage of the procedure which involves careful removal of the cement spacer in order to preserve the biological membrane and insertion of bone graft into the defect. The membrane is preserved throughout and is closed over the graft to help contain it and prevent the body resorbing the graft (where the body removes the graft).
The ideal bone graft to use is that harvested from the patients own body (autograft). For bone defects of up to 3cm the bone is normally harvested from the anterior iliac crest. For larger defects Mr Daurka and Mr Sinha regularly use the RIA technique, where bone graft is harvested from the canal of the femur or tibia.
Following the Masquelet second stage procedure the patient will normally require to be touch weightbearing for 6 weeks and then build up to full weight bearing by 12 weeks.
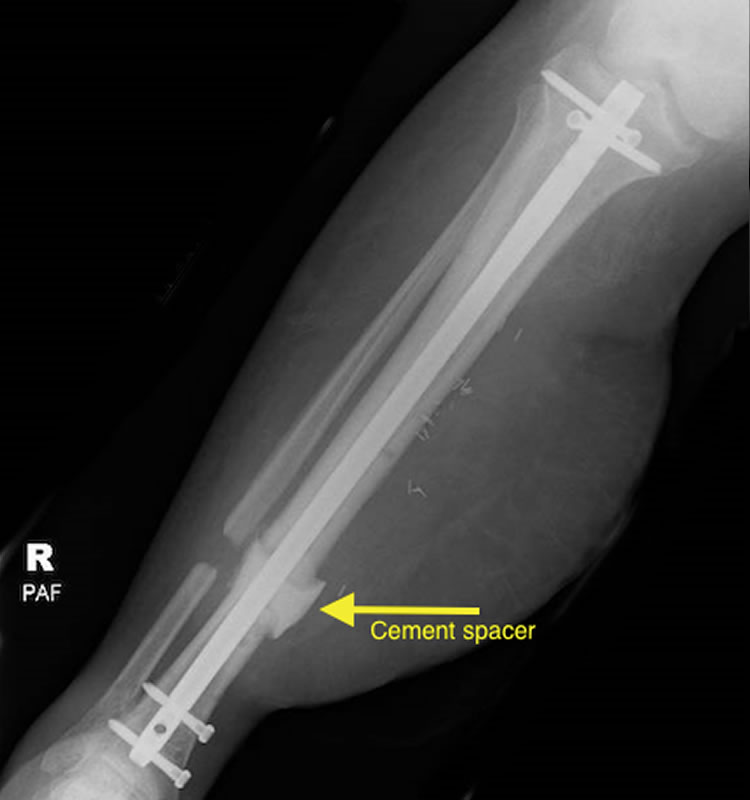
AP and lateral radiographs of tibia with cement spacer in tibial bone defect

AP and lateral radiographs tibia after second stage bone graft (RIA technique) with healing


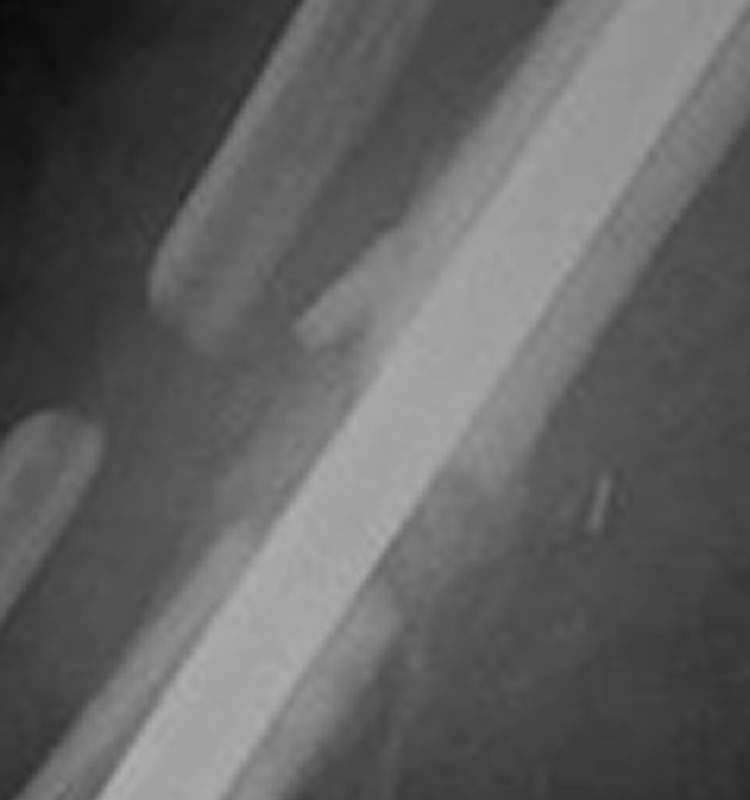
Zoomed in views showing bony bridging between bone graft and tibia