


ACL Reconstruction
ACL reconstruction is performed in patients with an ACL tear and symptoms of instability and/or associated meniscal tears requiring repair.
The most common graft option used is the patient's own medial hamstring tendons (the semitendinosus and the gracilis)- tissue from the same patient is termed autograft.
In some cases the semitendinosus can be used alone, if of sufficient length to be successfully tripled or quadrupled and a desired graft diameter of 8mm or more achieved in adults.
Other graft options include
- Patella tendon
- Quadriceps tendon
- Allograft (from another person)
- Synthetic graft (eg LARS ligament)
MRI scan of intra-substance ACL tear

Lateral femoral and tibial bone oedema and bone bruising secondary to ACL tear

Surgery
The surgery is performed under a general anaesthetic (patient asleep).
The procedure is performed with a tourniquet applied to the thigh.
The surgery is normally performed as a day case, though if combined with a meniscal repair then a one night stay may be required.
The surgery is performed using an incision at the front of the knee 5cm below the medial aspect of the knee joint to harvest the hamstring tendons.
The hamstring tendons are looped and sutured together to create the graft.
The knee joint is then prepared using an arthroscopic technique (keyhole) with 4 small incisions around the knee (3 at the front and one one the outer aspect of the lower thigh). Bone tunnels are prepared in the femur and tibia (into which the graft is passed).
The graft is secured into the bone tunnels in the femur and the tibia using a titanium suspensory femoral button and a tibial titanium screw. On some occasions a femoral screw may be used in preference or in addition to the suspensory button. If an 'all-inside' technique is used then a suspensory button is used to fix the graft on the femoral and tibial side.
Post operative rehabilitation
In case of an isolated ACL reconstruction the post operative rehabilitation pathway is:
- A brace is worn for the first three weeks and partial weight bearing with crutches is also recommended (to help reduce post operative swelling).
- Full range of movement is encouraged from day one.
- Full weight bearing is allowed from week three and a daily exercise bike regime on low resistance recommended.
- The use of a cross trainer can be introduced once you are able to complete 10 minutes on the exercise bike.
- Straight line running can begin at 6 weeks post operatively.
- For the first twelve weeks closed chain strengthening exercises of the quadriceps and hamstrings are performed.
- Open chain exercises are avoided for the first 12 weeks (as such exercises can stretch the repair and lead to early failure).
- Pool walking is encouraged after your surgical wounds have healed (ie after first surgical follow up consult).
- Swimming in the first twelve weeks MUST avoid leg kicks (again to avoid stretching the repaired ligament) and so must be performed gripping a float between the knees.
- Pivot specific drills are normally started at 6 months post operatively.
- Sport specific drills are commenced 10 months post operatively.
- Contact sports are normally not commenced until 12-14 months post operatively.
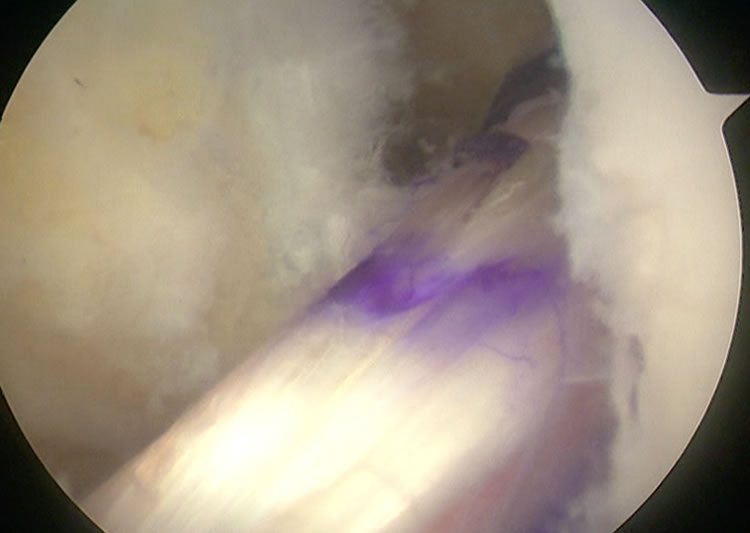
Intra-operative arthroscopic picture of reconstructed ACL with autologous hamstring
Post operative radiographs of ACL reconstruction

